Explore the complex world of dementia.
Dementia is a complicated condition. We aim to advance the understanding and empower researchers to impact the millions of lives affected by this destructive condition.
Dementia is a broad term referring to a progressive decline in cognitive abilities of the human brain leading to terminal disease.
The loss of cognitive functioning—thinking, remembering, and reasoning—and behavioral or movement abilities can eventually interfere with a person’s daily life and activities. Dementia ranges in severity from the mildest stage, when it is just beginning to affect a person’s functioning, to the most severe stage, when the person must depend completely on others for basic activities of daily living.
Contents
Epidemiology
The number of people living with dementia worldwide has already exceeded 46 million1 and is expected to increase dramatically to nearly 75 million people by 2030. Current estimates conclude that there will be over 9.9 million cases of dementia diagnosed annually worldwide, or, put slightly differently – one new case every 3.2 seconds.
With ever increasing patient numbers, the economic impact has already become a major burden on worldwide healthcare and social systems and will continue to increase for the foreseeable future. The total worldwide estimated cost of dementia in 2015 was $818 billion USD rising to $1 trillion in 2018 and $2 trillion USD by 2030. Mild cognitive impairment and dementia will have profound consequences for older adults, caregivers, the health care delivery system and society as a whole. Given this growing human and healthcare burden, the need to identify potential biomarkers for early detection and risk assessment remains a major focus.
Facts based on World Alzheimer Report 2015. Find more dementia facts and figures at Alzheimer’s Disease International: https://www.alz.co.uk/research/world-report-2015
Causes
The causes of dementia can vary, depending on the types of brain changes that may be taking place. Alzheimer’s Disease, discovered in 1906 by Dr. Alois Alzheimer2, is the most common type of dementia, affecting over 5 million people in the US alone.
Other dementias include Lewy body dementia, frontotemporal disorders, and vascular dementia. It is also possible for people to have mixed dementia—a combination of two or more types of dementia. For example, some people have both Alzheimer’s Disease and vascular dementia.
Some other conditions that may cause and/or accelerate onset of dementia include:
- Medication side effects
- Chronic alcoholism
- Tumors or infections in the brain
- Blood clots in the brain
- Vitamin B12 deficiency
- Some thyroid, kidney, or liver disorders
- Stroke
- Parkinson’s disease
- Huntington’s disease
- Traumatic brain injury
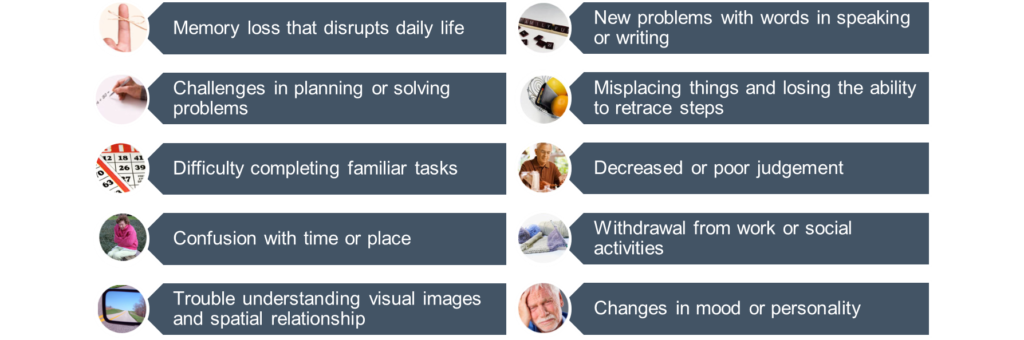
Symptoms
Symptoms of mild cognitive impairment or dementia vary from person to person and at least two impairments will be present. Symptoms can include:
Diagnosis
The diagnosis of dementia can be difficult, lengthy and expensive and usually requires the participation of a close family member to assist the individual with symptoms of dementia. Figuring out the cause of dementia requires a clinical-neuropathologic assessment. An evaluation could include:
- medical, symptom and family history
- neurological examination
- neuropsychological testing
- laboratory testing
- neuroimaging
- lumbar puncture
- genetic testing
Prior to advances in neuroimaging and laboratory testing, a definitive diagnosis was not likely to be made until autopsy.
Genetics
A genetic contribution to dementia is common but not always discovered. Significant research efforts are ongoing to identify/clarify the role(s) that certain genes and biomarkers play in the pathogenesis of dementia. Some research was accomplished with the completion of the human genome project and the knowledge that it brought. However, many areas of the genetic code have eluded analysis through conventional sequencing and next-generation sequencing methods. Recent advances in genotyping of these challenging regions can help us refine our understanding of the role of these genes in dementia.
Some of the genes that have been implicated in dementia are:
APOE
- Apolipoprotein E has been identified as a risk factor for the development of Alzheimer’s disease3. Of the three best-studied variants (E2, E3, or E4), individuals with E4 have a significantly higher risk of developing Alzheimer’s disease. Conversely, individuals with the E2 variant have a lower risk of developing Alzheimer’s disease.
TOMM40
- TOMM40 has an important role for the many individuals who are found to have the most common E3 variant of APOE. By determining the number of consecutive thymidine DNA bases one has in a particular region of the TOMM40 gene, scientists may further predict who is at a higher risk for developing Alzheimer’s disease and what age they may start to show symptoms.
- TOMM40 also has recently been associated with a role in the onset of cognitive decline in healthy elderly individuals without Alzheimer’s disease4. More research is needed to explore the important nature of this area of the gene.
The knowledge that these two markers can bring to individuals, healthcare systems, and society as a whole will enable valuable resources to be directed to the groups that are at the highest risk of developing this debilitating condition.
C9orf72
- The C9orf72 gene is the long sought after link between frontotemporal dementia, the 2nd most common form of dementia, and ALS (Lou Gehrig’s disease). The discovery of this gene region was hampered because it is very hard to detect the disease-associated expanded form that has hundreds or thousands of repeats of a 6 base DNA code, GGGGCC, instead of the normal handful of repeats.
Having the right tools to study this gene has led to a resurgence of research into FTD and ALS.
Other genetic markers that have been implicated in dementia are:
- PSEN1
- PSEN2
- APP
- MAPT
- VCP
- TDP43
- CHMP2B
- FUS
- GRN
- NOTCH3
- PRNP
- VCP
- TARDBP
Most cases of dementia seem to be sporadic, but even in sporadic cases, there might be an underlying genetic driver for the disease. Hence increased understanding of the whole genome will aid us in better understanding the prevalence, penetrance and pathogenesis of the disease.
Therapy
Approved medications to treat some forms of dementia are available, but there is no cure at this time. Three classes of medications have been approved to treat the most common form of dementia, Alzheimer’s disease.
- Acetyl-cholinesterase inhibitors (AChEs)
Aricept or donepezil
Exelon or rivastigmine
Razadyne or galantamine - N-methyl-D-aspartic acid receptor antagonists (NMDA)
Namenda or memantine - Selective serotonin reuptake inhibitors (SSRIs)
These medications can slow progression in early stages of the disease, but over time they may lose their ability to make a difference in symptoms or progression. The development of better diagnostic tools for dementia will help companies create faster and more effective therapies.
Many researchers are looking for better solutions for people affected with dementia. For more information on current or planned research, visit https://clinicaltrials.gov/.
Caregivers
“The huge majority of people with dementia have not received a diagnosis, and so are unable to access care and treatment. Even when dementia is diagnosed, the care provided is too often fragmented, uncoordinated, and unresponsive to the needs of people living with dementia, their careers and families. This is unacceptable.” −Glenn Rees, Chair of Alzheimer’s Disease International5
Having a family member affected with this debilitating disease creates deep respect for the millions of individuals who care for persons with dementia. Dementia takes a devastating toll on caregivers. Compared with caregivers of people without dementia, twice as many caregivers of those with this disease indicate substantial emotional, financial and physical difficulties6. To learn more, visit https://www.alz.org/facts/.
Our aim is to provide hope to those affected with this disease and to their family members by developing tools to empower researchers to find a cure.
Caregivers can seek out resources and interventions to better the outcome for the family as a whole, including7:
- Patient behavior management instruction
- Stress-coping management
- Caregiver-focused counseling and support groups
- Respite care
- Dementia care coordinators
- Community services
- Skill training to address safety, social support, problem behaviors, caregiver depression, and health
For more information on caregiver resources, please select from the list below.
Additional Resources
Alzheimer’s Disease International: +44 20 79810880
https://www.alz.co.uk/research/world-report
Alzheimer’s Foundation of America: 866-232-8484
http://www.alzfdn.org/?gclid=CP6NsuHRkNICFQUNaQodwuUKnQ
Alzheimer’s Association: 800-272-3900
http://www.alz.org/
Dementia Advocacy and Support Network
http://www.dasninternational.org/
Dementia Alliance International
http://www.dementiaallianceinternational.org/
Lewy Body Dementia Association: 404-935-6444
https://www.lbda.org/
The Association for Frontotemporal Degeneration: 866-507-7222
http://www.theaftd.org/
The Bluefield Project
http://www.bluefieldproject.org/ftd/links-and-resources
References
- World Alzheimer Report 2015. The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. August 2015.
- Alzheimer A. Über einen eigenartigen schweren Erkrankungsprozeβ der Hirnrincle. Neurol Central.1906;25:1134.
- Saunders AM et al. Association of apolipoprotein E allele epsilon 4 with late-onset familial and sporadic Alzheimer’s disease. 1993 Aug;43(8):1467-72.
- Yu L, et al. TOMM40 ‘523 variant and cognitive decline in older persons with APOE ε3/3 genotype. 2017 Feb 14;88(7):661-668.
- World Azheimer Report 2016. Improving Healthcare for People Living With Dementia: Coverage, Quality and Costs, Now and in the Future. September 2016.
- Alzheimer’s Association. 2017 Alzheimer’s Disease Facts and Figures. Alzheimers Dement 2017;13:325-373.
- Belle SH, Burgio L, Burns R, et al. Enhancing the quality of life of dementia caregivers from different ethnic or racial groups: a randomized, controlled trial. Annals Internal Medicine 2006; 145: 727–38.